Weight-loss surgery can be life-changing, but the story does not always end with the first operation. In some cases, Revisional Bariatric Surgery becomes part of the journey when the original procedure no longer works as expected, causes troubling side effects, or no longer matches a patient’s medical needs. For many people, this topic sounds intimidating at first. Yet when explained clearly, it becomes easier to understand why a second bariatric procedure may sometimes be considered and how it fits into the broader science of obesity treatment.
At Dr. Caynak, the conversation around bariatric care is approached with nuance, evidence, and realism. Obesity is not a simple issue of willpower, and surgical outcomes are not always perfectly linear. Bodies adapt. Hormones shift. Anatomy changes over time. This is why Revisional Bariatric Surgery is increasingly discussed in modern metabolic surgery literature not as a failure story, but as one possible chapter in long-term treatment.
In scientific terms, revision surgery refers to a procedure performed after an earlier bariatric operation. The goal may be correction, conversion, or improvement. Some revision operations are done to manage complications. Others are considered when weight loss is insufficient, weight regain becomes clinically significant, or quality of life is affected. The reasons vary, and so do the options.
Understanding Revisional Bariatric Surgery in Modern Obesity Treatment
Revisional Bariatric Surgery is an umbrella term used for a second bariatric operation performed after a previous weight-loss procedure. It is not a single technique. Instead, it includes a range of surgical strategies tailored to the anatomy, symptoms, and goals of the individual. In clinical practice, revision may involve repairing the original surgery, converting it into another procedure, or improving a prior result that has become less effective over time.
The rise of Revisional Bariatric Surgery reflects something important about obesity medicine: it is a chronic, complex condition. Long-term studies suggest that while bariatric surgery remains one of the most effective interventions for severe obesity, outcomes can differ widely between individuals. Some maintain strong results for many years. Others experience anatomical changes, metabolic adaptation, or behavioral challenges that alter those results. A revisional approach may then enter the discussion as a way to reassess the original pathway.
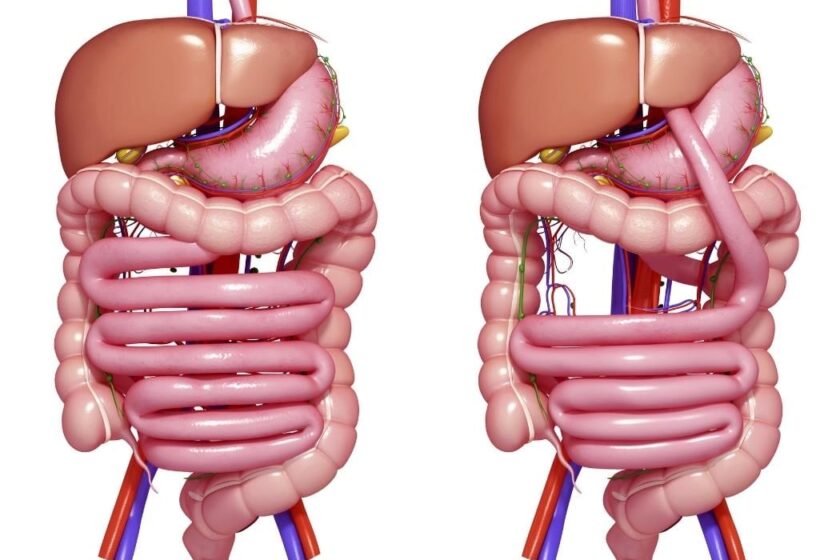
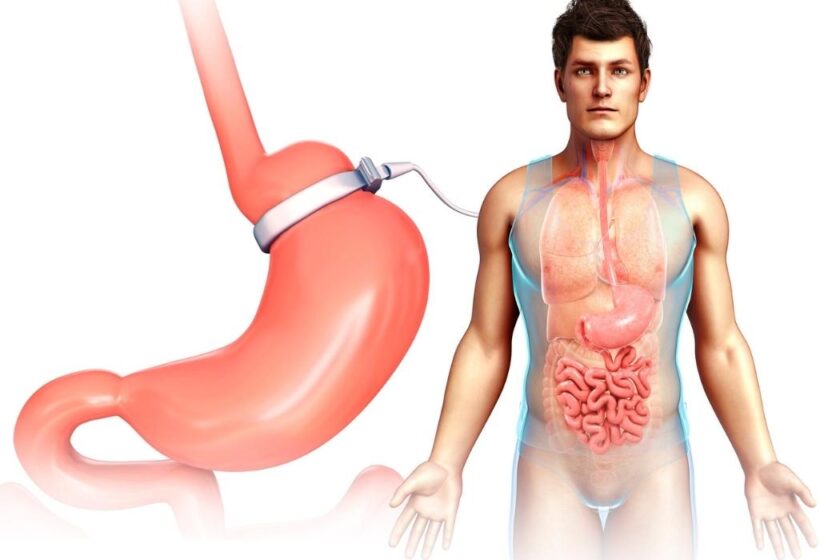
It is also helpful to separate myth from reality. Revision surgery does not automatically mean the first operation “failed.” In many situations, the first procedure may have helped for years before new issues appeared. For example, gastric bands may slip or erode, sleeve gastrectomy may be associated with reflux in some patients, or bypass anatomy may change functionally over time. Seen this way, Revisional Bariatric Surgery is less about blame and more about recalibration.
From an NLP-friendly perspective, the concept can be simplified into three categories:
- Correction – fixing a complication or anatomical issue
- Conversion – changing one bariatric procedure into another
- Optimization – improving a result when weight loss is inadequate or weight regain occurs
These categories often overlap, which is why comprehensive evaluation matters.
When Revisional Bariatric Surgery May Be Considered
There is no one-size-fits-all moment when Revisional Bariatric Surgery is considered. The need usually emerges from a combination of symptoms, test findings, weight trajectory, nutritional status, and overall quality of life. A second operation is often discussed only after a careful review of what has changed since the original procedure.
One common reason is insufficient weight loss. This refers to situations in which the expected metabolic or weight-related benefit from the first operation was limited. The causes can be varied. Sometimes anatomy plays a role. Sometimes the procedure chosen years earlier is now considered less effective for that person’s needs. In other cases, multiple biological and lifestyle factors interact in complex ways.
Another major reason is weight regain after an initial successful period. Research in bariatric follow-up suggests that some weight regain is not unusual over time, but the degree and significance matter. If regain becomes substantial and is linked with the return of obesity-related conditions, Revisional Bariatric Surgery may enter the conversation. That said, surgery is not the only lens through which weight regain is evaluated. Endocrine, behavioral, anatomical, and nutritional factors are often reviewed together.
A third reason involves complications or side effects from the original operation. These may include:
- Severe reflux after sleeve gastrectomy
- Band slippage or erosion after gastric banding
- Persistent vomiting or intolerance
- Ulcer-related concerns
- Anatomical narrowing or dilation
- Chronic discomfort affecting eating patterns
In these scenarios, the purpose of Revisional Bariatric Surgery may be less about the scale and more about restoring function, comfort, and safety.
Common Types of Revisional Bariatric Surgery
Because Revisional Bariatric Surgery is a broad field, the exact procedure depends heavily on the initial operation. A surgeon usually considers the current anatomy, symptoms, medical history, and long-term goals before discussing options. The revision route for one patient may be entirely different from that of another.
A few common examples are summarized below:
| Original Procedure | Possible Revision Path | Common Reason Discussed |
| Gastric band | Band removal or conversion to sleeve/bypass | Slippage, erosion, poor tolerance, limited weight loss |
| Sleeve gastrectomy | Conversion to gastric bypass | Reflux, insufficient weight loss, weight regain |
| Gastric bypass | Pouch/anatomy revision or distalization in selected cases | Weight regain, anatomical issues, functional problems |
| Older bariatric procedures | Conversion to newer metabolic surgery techniques | Complications, outdated approach, poor long-term tolerance |
These examples show why Revisional Bariatric Surgery is rarely a simple repeat of the first operation. It often requires a much more tailored strategy. Scar tissue, altered anatomy, and nutritional considerations can make revision more technically complex than primary surgery.
There is also a growing scientific interest in procedure selection. Some studies suggest that the reason for revision strongly influences which procedure may be considered most suitable. For instance, a person with severe reflux after sleeve gastrectomy may be evaluated differently from someone whose primary concern is weight regain. The “best” revision is therefore not universal. It depends on the problem being solved.
How Surgeons Evaluate the Need for Revisional Bariatric Surgery
The decision-making process around Revisional Bariatric Surgery is usually more detailed than the assessment for a first bariatric procedure. This is because the body has already undergone one major intervention, and the stakes of a second surgery can be different. In most modern bariatric programs, evaluation is multidisciplinary.
A typical assessment may include review of:
- Prior operative reports
- Endoscopy results
- Imaging studies such as contrast swallow tests
- Weight history over time
- Reflux symptoms or food intolerance
- Nutritional blood work
- Psychological and behavioral factors
- Existing obesity-related conditions
This process matters because symptoms can be deceptive. For example, weight regain may not always reflect a purely anatomical problem. In some cases, hormonal adaptation, eating behavior, stress, medication changes, or sleep-related disorders may contribute. That is why Revisional Bariatric Surgery is usually approached as part of a broader clinical investigation rather than as an automatic next step.
Another important aspect is expectation-setting. Revision procedures may help address certain medical or anatomical concerns, but they are not magic resets. Surgeons often discuss potential benefits, limitations, and risks in a realistic way. The science here is fascinating: outcomes after revision can still be meaningful, but they may be more variable than those seen after primary bariatric surgery. Honest framing is essential.
Benefits and Limitations of Revisional Bariatric Surgery
When appropriately selected, Revisional Bariatric Surgery may offer several potential benefits. It can improve symptoms such as reflux or vomiting, address mechanical problems, and in some cases support additional weight loss or renewed metabolic improvement. For individuals whose first procedure no longer aligns with their health needs, revision can represent a strategic adjustment rather than a dramatic detour.
There is also a quality-of-life dimension. Bariatric surgery is not only about kilograms lost. It can affect energy, mobility, eating comfort, sleep, social life, and confidence. If the original procedure causes chronic discomfort or no longer provides meaningful benefit, revision may be discussed as a way to improve daily functioning. In this sense, Revisional Bariatric Surgery sits at the intersection of metabolic science and lived experience.
Still, limitations deserve equal attention. Revision surgery is generally considered more complex than first-time bariatric surgery. Scar tissue, altered anatomy, and prior healing patterns may increase technical difficulty. Reported complication rates in revisional procedures can be higher than in primary cases, although this varies by center, surgeon experience, and procedure type. Recovery patterns may also differ from person to person.
For this reason, scientific discussions around Revisional Bariatric Surgery emphasize careful selection over aggressive intervention. Not every problem requires another operation. Sometimes dietary adjustments, medication review, endoscopic approaches, or structured follow-up may also play a role in management.
Risks, Recovery, and What Makes Revision More Complex
The phrase Revisional Bariatric Surgery often sounds straightforward, but technically it can be one of the more demanding areas of gastrointestinal surgery. A prior operation changes the surgical landscape. Tissues may be less predictable. Landmarks may be altered. Adhesions can make dissection more difficult. This complexity is one reason why experience and planning are so important.
Potential risks vary depending on the original surgery and the revision being discussed, but may include bleeding, leaks, infection, stricture, nutritional issues, or persistent gastrointestinal symptoms. It would be misleading to present these as inevitable outcomes; many patients recover well. However, the scientific literature consistently suggests that revisional procedures require particularly thoughtful preoperative assessment and postoperative monitoring.
Recovery after Revisional Bariatric Surgery also depends on the procedure performed. Some patients may experience a relatively familiar path, especially if they already understand bariatric dietary stages and follow-up routines. Others may find the second experience emotionally different from the first. Expectations can be more layered. There may be hope, frustration, caution, or even relief.
This emotional dimension should not be underestimated. Revision is not only a technical event; it is often the result of a long and complicated relationship with weight, health, and previous treatment. That is why good bariatric care tends to combine surgical expertise with clear communication and long-term support.
Life After Revisional Bariatric Surgery: Long-Term Perspective
The long-term view of Revisional Bariatric Surgery is less about dramatic promises and more about sustainable management. Outcomes can include symptom relief, renewed metabolic benefit, and improved treatment alignment, but long-term success still depends on many factors beyond the operating room. Follow-up remains central.
Nutrition is one key area. Since many revisional procedures affect digestion and absorption differently, postoperative monitoring often becomes especially important. Protein intake, vitamin levels, iron status, B12, folate, calcium, and vitamin D are common areas of attention in bariatric follow-up literature. This does not mean every patient develops deficiencies, but it explains why structured monitoring is part of the conversation.
Another long-term theme is adaptation. Bodies respond over time, and habits evolve. The most useful way to think about Revisional Bariatric Surgery may be as one tool in chronic disease management rather than as a final finish line. This perspective is both scientific and humane. It respects biology, acknowledges complexity, and avoids simplistic narratives.
At Dr. Caynak, this subject is best understood not through fear, but through clarity. A revisional procedure may be considered when anatomy, symptoms, or outcomes suggest that the original operation is no longer the ideal fit. The important question is not whether revision sounds dramatic. The important question is whether the full clinical picture supports it.
Why Revisional Bariatric Surgery Requires Individualized Thinking
Revisional Bariatric Surgery occupies a unique place in obesity treatment. It is part surgical science, part metabolic strategy, and part long-term problem solving. It may be considered after limited weight loss, significant weight regain, anatomical changes, or quality-of-life concerns linked to a previous bariatric procedure. Yet its meaning is never generic. Every revision story begins with a specific reason.
What makes this field so compelling is its honesty. It recognizes that obesity treatment is dynamic, not static. It accepts that a procedure that once worked well may later require adjustment. And it highlights a central truth of modern medicine: successful care often depends on reassessment, not perfection.
For readers exploring the topic, the key takeaway is simple. Revisional Bariatric Surgery is not merely a second surgery. It is a carefully evaluated response to changing medical realities. When discussed thoughtfully, it becomes less mysterious and more understandable a precise tool used in selected circumstances, guided by anatomy, symptoms, evidence, and long-term goals.