When it comes to male chest appearance, distinguishing between Gynecomastia and fat can be more challenging than it appears. Many men notice changes in their chest and assume it’s simply excess weight, but these conditions are fundamentally different, each with unique causes, textures, and implications. Recognizing the differences helps clarify misconceptions and supports informed decisions about health and fitness.
Gynecomastia involves glandular tissue development, while fat accumulation is related to overall body composition. Understanding these distinctions allows men to approach their chest appearance with clarity and confidence.
Understanding Gynecomastia and Fat in Men
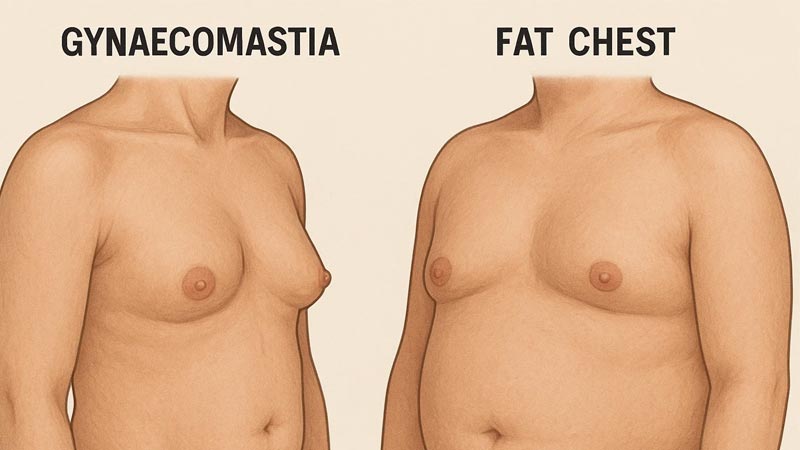
Gynecomastia and Fat may appear similar at first glance, but the underlying structure is completely different. Gynecomastia refers to the enlargement of glandular breast tissue in males, often due to hormonal imbalances, medications, or underlying medical conditions. On the other hand, fat accumulation in the chest, also called pseudogynecomastia, is purely the deposition of adipose tissue and is usually linked to weight gain.
From a tactile perspective, Gynecomastia and Fat feel different. Glandular tissue is firmer and more centralized around the nipple, whereas fat is softer and spread across the chest area. This distinction is important for men trying to assess their chest composition at home or for physicians conducting a physical exam.
Studies show that approximately 30-40% of adult men experience some degree of Gynecomastia and Fat during their lifetime, with varying causes ranging from puberty to aging. While fat in the chest can be reduced with general weight loss strategies, glandular tissue requires a more nuanced approach for change.
Causes Behind Gynecomastia and Fat
The root causes of Gynecomastia and Fat differ substantially. Hormonal fluctuations, particularly increased estrogen or reduced testosterone, are major drivers of gynecomastia. Other contributors include medications such as anti-androgens, steroids, or certain cardiovascular drugs. In contrast, chest fat develops due to caloric surplus, sedentary lifestyle, and genetic predisposition to store fat in the upper body.

Interestingly, some men experience a combination of both conditions, which can make the distinction more challenging. This overlap often leads to confusion when evaluating whether lifestyle changes alone will improve chest appearance.
| Cause Type | Gynecomastia | Chest Fat |
| Hormonal | Estrogen/Testosterone imbalance | Rarely hormonal |
| Lifestyle | Minor influence | Major factor (diet, activity) |
| Texture | Firm, rubbery | Soft, diffuse |
| Treatment Impact | May require medical intervention | Weight loss & exercise |
The table above clearly illustrates that while both conditions may coexist, they have fundamentally different origins and manifestations, highlighting the importance of accurate assessment.
Physical Differences Between Gynecomastia and Fat
The physical characteristics of Gynecomastia and Fat differ in several measurable ways. Gynecomastia is characterized by proliferation of glandular tissue beneath the areola, often presenting as a firm, rubbery mass. Adipose tissue accumulation in the chest, in contrast, is softer and more diffuse, distributed over the pectoral region rather than concentrated around the nipple.
Clinical observations indicate that gynecomastia frequently exhibits asymmetry, affecting one breast more prominently than the other. Fat deposition tends to be more symmetric and correlates with overall body adiposity. The structural differences between glandular and adipose tissue are significant for diagnostic purposes and for determining the appropriate management strategies.
Diagnostic Assessment of Gynecomastia and Fat
Accurate differentiation between Gynecomastia and Fat requires clinical evaluation, often including palpation and imaging studies. Ultrasonography can distinguish between glandular tissue and adipose tissue, while mammography may be used in atypical presentations or when malignancy must be excluded.
Physical examination remains a primary tool: glandular tissue is typically discrete and firm with a defined border beneath the nipple, whereas fatty tissue is soft, compressible, and lacks a clear demarcation. Clinical guidelines recommend assessing hormonal levels when gynecomastia is suspected, particularly in cases with rapid onset, pain, or unilateral enlargement.
| Parameter | Gynecomastia | Chest Fat |
| Tissue Type | Glandular | Adipose |
| Consistency | Firm, rubbery | Soft, pliable |
| Symmetry | Often asymmetric | Usually symmetric |
| Diagnostic Imaging Utility | Ultrasound/Mammography | Limited; mostly visual |
| Hormonal Assessment | Recommended in non-obese individuals | Generally not indicated |
Influence of Lifestyle and Body Composition
The impact of lifestyle on Gynecomastia and Fat differs significantly. Fat deposition in the chest is strongly correlated with total body fat and responds to caloric restriction and structured exercise programs. Reduction of subcutaneous adipose tissue can be quantified using body composition analysis, such as dual-energy X-ray absorptiometry (DEXA) or bioelectrical impedance.
In contrast, glandular proliferation associated with gynecomastia is less responsive to caloric deficit or resistance training. Evidence suggests that spontaneous regression may occur in cases related to puberty or transient hormonal fluctuations, but persistent gynecomastia often requires pharmacological or surgical intervention for resolution.
Clinical Misconceptions About Gynecomastia and Fat
There exist several prevalent misconceptions regarding Gynecomastia and Fat. One common error is the assumption that all male breast enlargement is due to excess adipose tissue. Studies indicate that up to 65% of male breast enlargements in certain populations are attributable to glandular proliferation, independent of overall body fat.
Another misconception is that targeted pectoral exercises can reduce glandular tissue. While exercise improves muscular definition and may reduce overlaying adipose tissue, it does not affect glandular tissue. Misinterpretation of these distinctions can lead to inappropriate management and delayed clinical evaluation.
Long-Term Considerations in Gynecomastia and Fat
Long-term management and monitoring of Gynecomastia and Fat depend on the underlying tissue type. Fat accumulation in the chest generally responds to sustained lifestyle interventions, including dietary regulation and structured physical activity. Longitudinal studies demonstrate that reductions in total body fat result in proportional decreases in subcutaneous chest fat.
Glandular tissue, in contrast, may persist without regression. Research indicates that persistent gynecomastia can be associated with endocrine disorders, medication side effects, or systemic conditions. Therefore, clinical evaluation is advised for cases where chest enlargement does not resolve with weight normalization or presents with pain, rapid growth, or asymmetry.
Potential Interventions for Gynecomastia and Fat
Interventions differ based on tissue composition. Chest fat reduction primarily involves caloric restriction, aerobic exercise, and resistance training targeting the pectoral region. Quantitative assessments using body composition metrics can objectively track reductions in adipose tissue over time.
Gynecomastia treatment may require pharmacologic agents that modulate hormonal activity or surgical excision of glandular tissue in persistent cases. Current guidelines recommend surgery primarily for long-standing or symptomatic gynecomastia. Clinical studies confirm that differentiating Gynecomastia and Fat prior to intervention improves treatment efficacy and reduces unnecessary procedures.
Implications for Clinical Practice
Gastric Sleeve procedures can influence chest appearance in men by reducing overall body fat, which may help differentiate fat accumulation from true Gynecomastia. Accurate identification of chest enlargement remains crucial, as Gynecomastia involves glandular tissue and requires different clinical management. Integrating physical examination, imaging, and endocrine evaluation ensures evidence-based care. Understanding the underlying cause allows clinicians to guide patients regarding realistic outcomes of lifestyle changes versus medical or surgical treatments.